42Yr old female, with fever and vomiting
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box are welcome.














Provisional diagnosis -Fever under evaluation
NAME: Meghana Muddada
Roll no: 90
Batch: 2017
Case history:
A 42 y /F came to the casualty with complaints of fever , nausea , vomitings, constipation , generalised weakness since 7days ; burning micturition since 1day
HOPI-
Patient was apparently asymptomatic 1week back when she developed fever, which is intermittent, not associated with chills , rigors , associated with generalised weakness. Its also associated with nausea , constipation , passing flatus.
Patient also complaints of nausea associated with one spontaneous episode of vomiting. Following which the patient stimulated vomiting by herself whenever she feels nauseating.
No c/o loose stools.
C/o burning micturition since 1day .
Dry cough since 1day
No c/o sputum , SOB , bleeding manifestations.
Not a k/c/o DM , HTN ,TB, Asthma , CAD
Personal history -
Diet - mixed
Appetite - Decreased
Sleep - Adequate
Bowel and bladder movements-- constipation
Rashes and itching on eating non veg .
No addictions .
Family history - not significant.
On Examination -
GENERAL EXAMINATION
Patient is conscious
Oriented
Co-operative
Moderately built
Well nourished
Palor - absent
Icterus absent
Cyanosis – absent
Clubbing – absent
Pedal edema – absent
No lymphadenopathy
VITALS:
PULSE: rate : 100bpm, regular rhythm, normal volume, and character, felt in all peripheral pulses, no radioradial delay, condition of vessel wall normal.
BLOOD PRESSURE: 110/70mm of Hg measured in the left Upper limb with the patient in supine position
RESPIRATORY RATE: 26/min, type-thoracoabdominal.
TEMPERATURE: 98°F measured in the Axilla
SYSTEMIC EXAMINATION:
ABDOMINAL EXAMINATION:
INSPECTION:
Shape – Generalized fullness due to fat
Umbilicus – Position: central, Shape- inverted
Skin – normal with no scars, or sinuses,
no dilated veins
Abdominal wall moves with respiration, no visible gastric peristalsis,no visible intestinal peristalsis
PALPATION:
No tenderness or superficial raise in temperature.
On deep palpation, no significant organomegaly
Measurements - Abdominal Girth: 90cms,
Distance between the Xiphisternum-Umbilicus is 18cms and Umbilicus-Pubic Symphysis is 22cms
No renal angle tenderness
PERCUSSION:
Liver span: 12cms
AUSCULTATION:
Bowel sounds – audible in right iliac fossa
Bruit – Absent
CNS EXAMINATION:
Higher mental functions intact
Cranial nerve examination normal
Motor examination:
Bulk: normal in all muscles Tone: normal in all muscles Power 5/5 in all muscles
Reflexes: superficial and deep reflexes present
Sensory system:
Pain, temperature, touch, vibration sensations are present,
Two point discrimination, tactile localisation present
Cerebellar functions normal
RESPIRATORY SYSTEM:
INSPECTION:
Upper respiratory tract: no significant findings
Lower respiratory tract:
Position of trachea is midline
Chest symmetrical
Movement of chest: equal on both sides with respiration
No visible dilation of veins no scars ,sinuses
PALPATION:
Trachea is in midline
Chest expansion: Normal and equal on botgh sides
Vocal fremitus: equal on both sides
PERCUSSION:. Right Left
Clavicular percussion. resonant on both sides
Kronig’s isthumus. resonant on both sides
Infraclavicular. resonant on both sides
Mammary. resonant on both sides
Axillary. resonant on both sides
Infraaxillary. resonant on both sides
Suprascapular. resonant on both sides
Infrascapular. resonant on both sides
Upper/mid/lower
interscapular region. resonant on both sides
AUSCULTATION:
Breath sounds: Normal Vesicular Breath sounds heard in all auscultatory areas.
No added breathe sounds
Vocal resonance:
Clavicular percussion resonant on both sides
Kronig’s isthumus. resonant on both sides
Infraclavicular. resonant on both sides
Mammary. resonant on both sides
Axillary. resonant on both sides
Infraaxillary. resonant on both sides
Suprascapular. resonant on both sides
Infrascapular. resonant on both sides
Upper/mid/lower
interscapular region. resonant on both sides
CARDIOVASCULAR EXAMINATION:
JUGULAR VENOUS PULSE:
INSPECTION:
Chest wall elliptical in shape and symmetrical,
Precordial bulge absent
Dilated veins, scars, sinuses absent
Apical impulse not seen
Pulsations – no visible pulsations
PALPATIONN:
Apical impulse – normal in left 5th ics , 1cm medial to midclavicular line.
No parasternal Heave or thrills
PERCUSSION:
AUSCULTATION:
S1 S2 heart sounds are heard
No abnormal heart sounds heard.
CLINICAL IMAGES:
X-ray:
Fever chart:
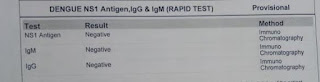
INVESTIGATIONS:
UTI ?
Treatment -
IVF -NS,RL,DNS @75ML)HR
INJ PANTOP 40MG IV OD
INJ ZOFER 4MG IV SOS
INJ OPTINEURON 1AMP IN 100ML NS IV OD
INJ NEOMOL 1GM IV SOS (IF TEMP >101°F)
TAB DOLO 650 MG PO SOS
SYP LACTULOSE 10ML PO H/S


Comments
Post a Comment